Attia Statins
However, like all lipids (fats), cholesterol is insoluble in water-based plasma and needs a hydrophilic peptide (a so-called apoprotein) to enwrap and transport the lipids in particles called lipoproteins. Though various classes of lipoproteins exist, only those containing apoB, short for apolipoprotein B, can enter, aggregate, and be oxidized within an arterial wall, which in turn promotes an inflammatory response, the development of plaques, and thus, ASCVD.Low-density lipoproteins (LDLs), each of which has a single apoB molecule, make up 90-95% of all apoB-containing lipoprotein particles due to their prolonged plasma residence time relative to other apoB particles, and therefore, LDL cholesterol (LDL-C) is frequently used to estimate apoB. How do statins help? LDL-C concentration of <100 mg/dL is considered “optimal” Statins reduce the amount of circulating apoB through the inhibition of hepatic (liver) cholesterol synthesis Seven statin medications currently have approval from the Food and Drug Administration for LDL reduction: atorvastatin fluvastatin lovastatin pitavastatin pravastatin rosuvastatin simvastatin. An individual who achieves an LDL-C of 75 mg/dL after decades of creeping up to a peak of 160 mg/dL is still at far greater ASCVD risk than an individual who has always been at 75 mg/dL. Why? Because the progression of ASCVD is a function of both apoB concentration and duration of exposure. It's like smoking SIDE EFFECTS Like any medication, statins are not completely without possible adverse effects, including gastrointestinal distress, brain fog, and dose-related muscle pain. The most common side effect, muscle pain, has a variety of causes, and in a meta-analysis of randomized controlled trials, there was around a 7% relative increase in this symptom between the control and intervention groups during the first year, corresponding to an absolute additional rate of muscle pain or weakness of 11 events per 1000 person-years. After the first year, the statin groups showed no increase in muscle-related symptoms compared to the control groups. More potent statins, such as atorvastatin or rosuvastatin, had slightly higher rates compared to more moderate or less potent statins. Depending on the severity of symptoms, switching to a nonstatin therapy, a statin with lower rates of adverse effects, or a lower dose statin (with a combination of other LDL-lowering medications) may be an option. Several alternative therapeutic options to statins – such as PCSK-9 inhibitors or bempedoic acid – are also effective in combatting high LDL. Other more serious side effects include rhabdomyolysis, elevated liver enzymes, and the development of type 2 diabetes. Rhabdomyolysis is a severe condition that causes skeletal muscle breakdown, and in such cases, statin use should be discontinued. Less than 0.05% of patients on statins develop rhabdomyolysis, but concurrent use of certain antibiotics or other drugs such as fibrates increases this risk. Statin therapy is associated with elevated hepatic transaminases in anywhere from 1-3% of patients. Most of these cases are asymptomatic and do not require discontinuation of therapy; however, statin use in patients with acute liver disease is contraindicated for this reason. Elevated blood glucose is another possible side effect of statin use, and the onset or progression of type 2 diabetes is another reported effect of statins. The exact mechanism for this development is not currently known, but there are several pathways of glucose metabolism that may be affected. The excess risk of new-onset type 2 diabetes from any statin is estimated to be 9-12% higher when compared to placebo, and in large meta-analyses, this outcome is a moderate effect. However, the risk of new-onset diabetes is statin-specific: atorvastatin, rosuvastatin, and simvastatin have reported dose-dependent excess risks from 10% to upwards of 40% depending on the study. Some of the variability between risks reported is due to heterogeneity in statin dose and duration of treatment, as well as the population itself – one of the strongest risk factors for a new diagnosis was metabolic syndrome or pre-diabetes at baseline. In other words, those most likely to be pushed over the edge already had some degree of metabolic dysfunction.
Posted in Uncategorized
VO2 Max
You gotta jack the heart rate up.

HIIT, Tempo workouts.
20 minute over all. Divided as follows:
Posted in Uncategorized
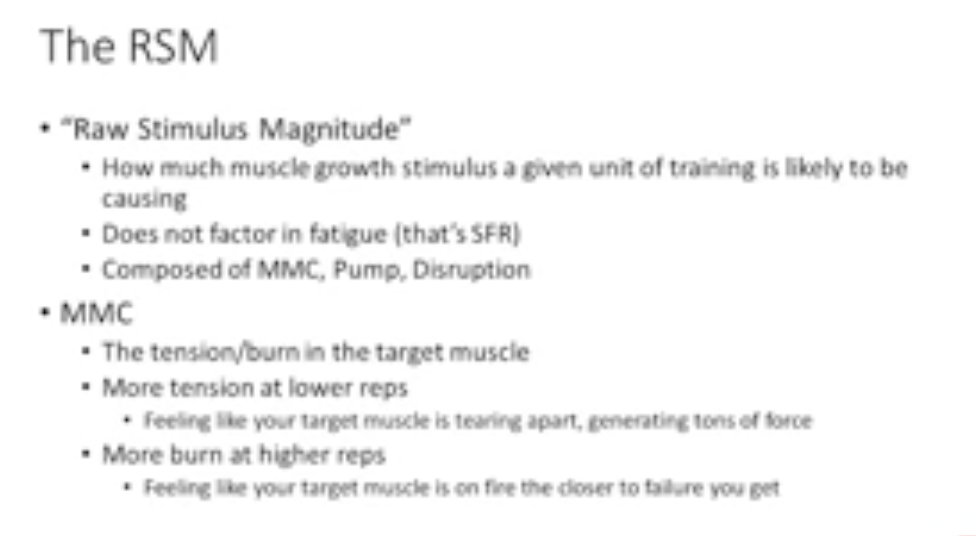
Mind Muscle Connection
Intentionally focus on squeezing and targeting the muscles.
Posted in Uncategorized
Be in a Deficit and Be Active
That’s it.
Youre eating too many carbs? Well, be in a deficit, and remain active. And see if you can sustain that.
Drinking too much? Go ahead, drunk you weak ass but be in a fucking deficit. If you cannot do that, then don’t fucking drink.
Eating too many sweets? Eat them bro. But be in a deficit. Otherwise, fuck off.
Deficit causing you to not be able to be Be Active? Fuck that bro — eat better quality food then. But be in a deficit.
That is is. Sustain the calorie restriction until the end of the year. Every week needs to be balanced to be below the deficit. Every fucking week. Start counting.
Posted in Uncategorized
Losing weight is HARD
This really is so fucking hard. It is the hardest thing I have ever done. Why is it so hard?
The reason is that it is a long process that interferes with you mind and schedule. You can’t just set it and forget it. It requires daily mental and physical cycles for a sustained period of time. And, due to the long “holding horizon”, you sometimes don’t even know if you are making progress or not.
Weight loss Sharpe Ratio
What I need is a high Sharpe strategy. This means I want a reliable way that can consistently make me lose weight. That consistency will have to come from deficit + light workout.
Why is it so hard to keep consistent?
The tail events that cause me to deviate from this strategy include things like:
- Fucking boredom. Sometimes I want to go out and just party.
- Uncontrolled environment for meals, with family, gf, etc.
- A massive tail event that causes me to just stop giving a shit.
- Not tracking in Lose It
- Stress, late nights at work, etc.
Each of these tail events needs to be curtailed. Every moment, every second of my life has to have a gate — a buffer — to stop me from descending down into hell. I cannot let time go by and not make progress on this goal dude. No, I cannot do that.
Keep it simple
There are so many tail events, so many things to balance, etc etc etc etc etc.
*Deep breadth* Just take a step back and keep it simple. Be in a deficit, and remain active. That’s it.
Posted in Uncategorized
Obesity is a disease
So cure it RAPIDLY.
I know this. I felt it. So I don’t know why I lost track of that goal.
I guess I was focussed a bit on the marathon stuff. That’s all good an all, but don’t loose track of this. This is the number you need to track. Weight. That’s your optimization function for now.
Workouts are good to increase calorie burn. Weight is the ultimate goal.
I have fucked up so far but not anymore. I am just so tired of not doing it.
Binge watching tv shows? use that idea for weight loss. Just do it rapidly now. Fuck it. I know it is mentally taxing, but fuck it, we need to do it.
[0] Muscle mass ain’t shit : https://www.nih.gov/news-events/news-releases/calorie-restriction-humans-builds-strong-muscle-stimulates-healthy-aging-genes
Posted in Uncategorized
Shoulder external rotation mobility
I finally have a name for the issue I have pretty much always had in my left shoulder: external rotation limitation!
Left shoulder external rotation
God dammit. Took me so long to understand this.
Use a beginners mind, challenge all conventions.
Anyway, I want to solve this.
- Supine progression
- Wall raises
Posted in Uncategorized
Mobility
Hearing more and more about this. From people like attia too.
Video 1
1) World’s Greatest Stretch: Engage multiple muscle groups with this dynamic stretch that targets the hips, hamstrings, and upper body.
2) Prayer Stretch: Release tension in your upper back, shoulders, and chest with this soothing stretch.
3) Eccentric Curl-Up: Strengthen your core and promote spinal stability with this controlled movement.
4) Goblet Squat Stretch: Enhance hip and ankle mobility while improving your squat form with this stretch.
5) KB Windmill: Develop shoulder and core strength as well as improve rotational mobility with this kettlebell exercise.
Video 2
1. SHOULDER – EXTERNAL ROTATION
2. SHOULDER – INTERAL ROTATION
3. CHEST
4. THORACIC
5. LOWER BACK
6. GLUTES / HIPS
7. ADDUCTORS / KNEES
8. HAMSTRINGS / HIPS
9. CALF / ANKLE
Posted in Uncategorized
Muscle workout correlated with age!
Contrary to what I used to think, you need to increase your exercises, especially weight lifting.
The Mid Life Muscle Crisis
- People focus on diet
- BUT HOLY SHIT SKELETAL MUSCLE IS FUCKING IMPORTANT
- Unhealthy muscles
- Over fat vs. Under Muscle
Muscle is the organ of longevity
Obesity is a disease of the MUSCLE. Muscle is MEDICINE. It sucks up the glucose. It is the metabolic sync.
MUSLCE directly correlated with LONGEVITY
How?
- Protein intake
- Resistance training
- Three days a week until exhaustion
Posted in Uncategorized
| The Cost of Cowardli… on Courage |
